PMS Symptom Support: What the Evidence Actually Supports
PMS supplement advice gets messy because every symptom gets marketed like it needs a different miracle. The more useful approach is narrower: start with the few options that actually have decent evidence, match them to your symptom pattern, and track over at least 2 to 3 cycles instead of expecting a dramatic shift in one month.
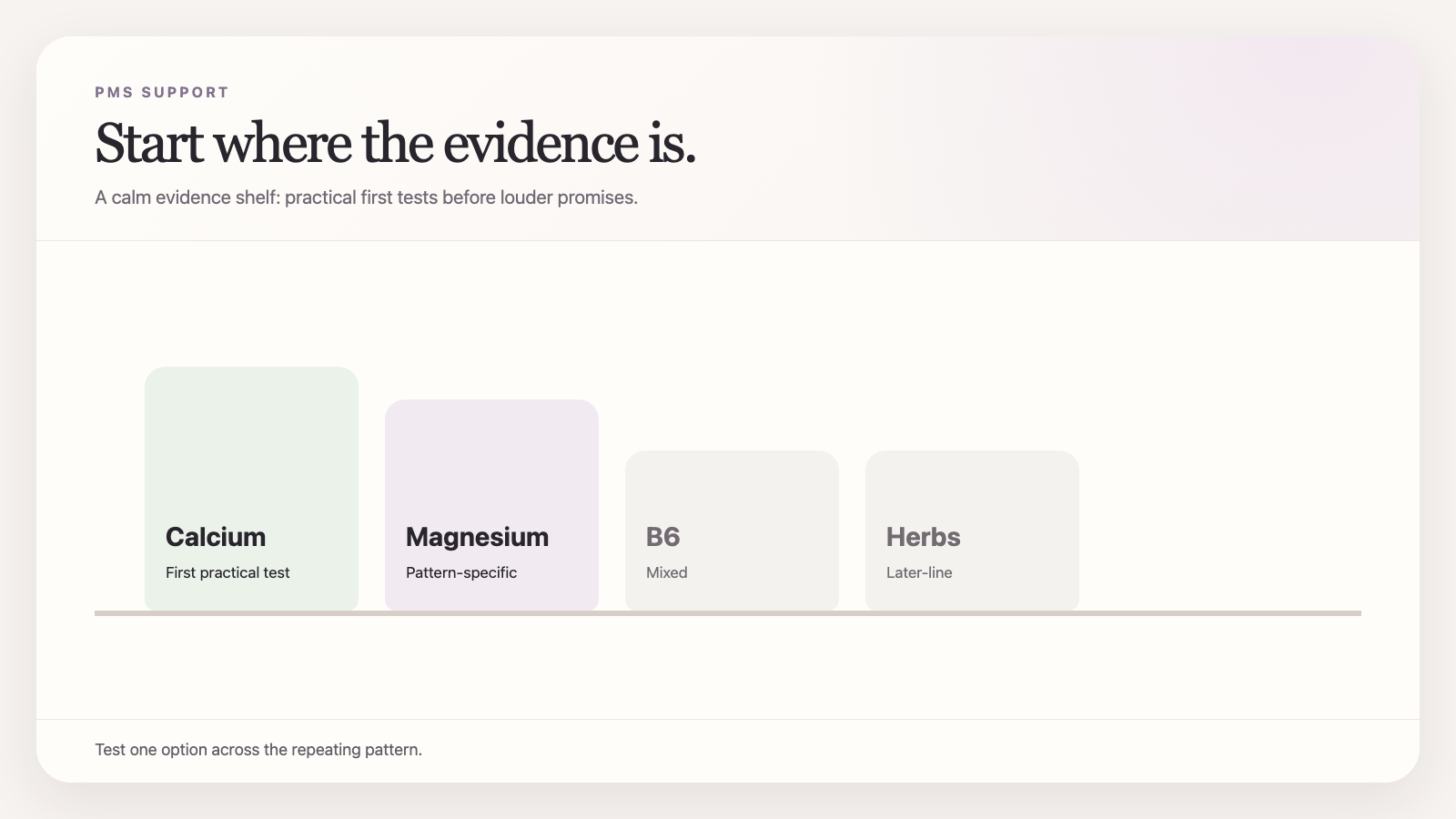 PMS is where the supplement aisle gets loud. The evidence is quieter and more useful.
PMS is where the supplement aisle gets loud. The evidence is quieter and more useful.
PMS is an easy category to oversell because the problem is real, recurring, and emotionally expensive.
If you get mood changes, bloating, breast tenderness, headaches, food chaos, sleep disruption, or the familiar sense that your nervous system became less cooperative for one week every month, you are motivated to try something. That is how the supplement market gets away with turning weak ideas into confident bottles.
The evidence-backed version is less sexy:
- there is no single supplement that fixes every version of PMS
- a few options have better evidence than the rest
- the right read usually takes 2 to 3 cycles, not one heroic month
Start with the highest-confidence options
Calcium
Calcium is the cleanest place to start because it has some of the best evidence in the PMS supplement category.
Older but still important randomized trials found that 1,000-1,200 mg/day reduced overall PMS symptoms over multiple cycles compared with placebo. Reviews of dietary supplements and herbal remedies for PMS repeatedly come back to the same conclusion: calcium is one of the few options with meaningfully better support than most of the field.
That does not mean every woman with PMS is calcium-deficient. It means calcium is one of the rare interventions where the category evidence is strong enough to justify a real experiment.
Best fit:
- broad PMS symptom clusters
- mood + physical symptoms together
- cyclical symptoms that reliably show up late-luteal
Magnesium
Magnesium is not as strongly supported as calcium overall, but it remains plausible, especially when PMS overlaps with tension, headaches, irritability, or worse sleep.
Some trials and reviews suggest benefit, but the quality is not as clean and the effect probably varies more by symptom pattern. Magnesium makes the most sense when the late-luteal week feels physically and neurologically noisy rather than just emotionally miserable.
Best fit:
- tension
- worse sleep
- headaches
- stress-fragile luteal weeks
Vitamin B6
Vitamin B6 has been in the PMS conversation forever, mostly because it plausibly intersects with neurotransmitter pathways and some women report feeling better on it. The problem is that evidence quality is mixed and dosing can become stupid fast if people self-prescribe aggressively.
It is not my first-choice starting point because calcium is cleaner, and magnesium is usually easier to justify symptom-wise. But it is still part of the evidence-based discussion.
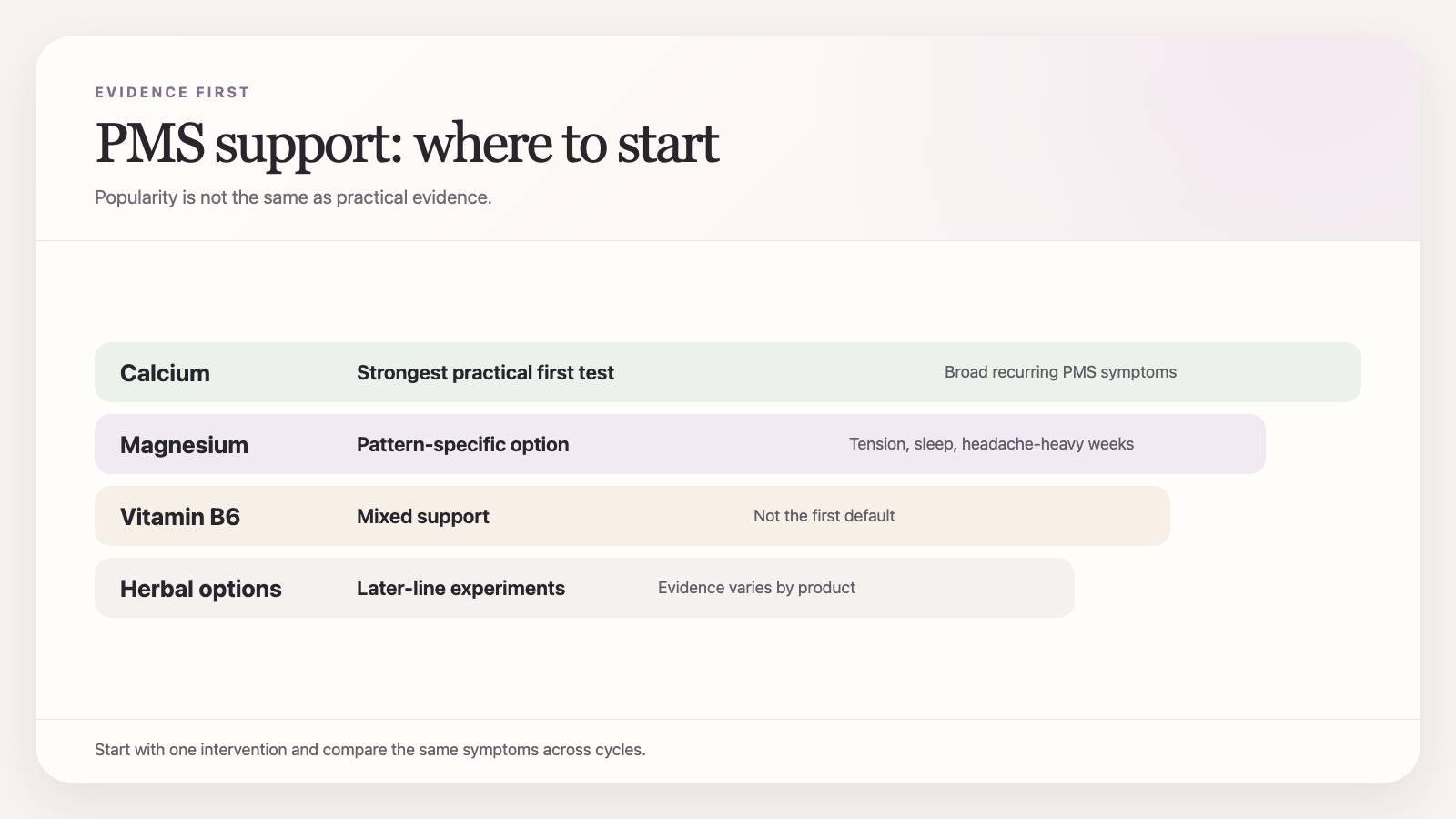 Evidence narrows the first experiment: start with the options that have earned first billing.
Evidence narrows the first experiment: start with the options that have earned first billing.
What about herbs?
Herbal medicine for PMS is a giant mixed bag.
The broader systematic review and meta-analysis on herbal medicine and nutritional supplements for PMS suggests some herbal options may help, but trial quality remains uneven. Translation: possible, but not reliable enough to recommend with the same confidence as calcium.
That does not make herbs fake. It makes them second-line experiments after the simpler options with better support.
If your symptom picture is very specific, a more targeted herb experiment may make sense later. It just should not be where the average woman starts.
The mistake: treating PMS like one symptom
PMS is not one thing. That is why supplement advice gets sloppy.
One woman has mainly:
- bloating
- breast tenderness
- headaches
Another has mainly:
- irritability
- low mood
- anxiety
- sleep disruption
Another has both.
When a supplement study shows "overall symptom improvement," that can still mask important differences in which symptoms moved most. So the smarter approach is to match the experiment to the pattern instead of asking for a universal winner.
A reasonable evidence-first approach
If you want a practical sequence:
Step 1: Track the pattern for 1 cycle
Track:
- start day
- end day
- physical symptoms
- mood symptoms
- sleep
- appetite/cravings
This tells you whether you actually have a predictable PMS window or whether you are lumping together random hard weeks.
Step 2: Start with one of the clearer options
- Calcium if symptoms are broad and recurring
- Magnesium if the pattern is more tension/sleep/headache-heavy
Step 3: Give it 2 to 3 cycles
This is where impatience ruins the read.
PMS supplements are not one-night interventions. The pattern is monthly, so your evidence window has to be monthly too.
![]() A monthly pattern needs more than one month before you call an intervention a winner or a failure.
A monthly pattern needs more than one month before you call an intervention a winner or a failure.
Do not forget the obvious non-supplement levers
This is the part supplement content hates because it does not sell as well:
- worse sleep can amplify PMS symptoms
- late-luteal alcohol often lands harder
- inconsistent eating can make cravings and mood volatility worse
- training load sometimes needs small adjustments in the worst week
None of that means supplements are useless. It means they work inside a system.
If the system is chaos, the capsule gets blamed for failing at a job it was never meant to do alone.
When to stop calling it PMS and look deeper
If symptoms are severe, disabling, or feel more like PMDD than ordinary PMS, do not reduce the whole thing to supplement shopping.
Likewise if symptoms are paired with:
- very heavy bleeding
- severe fatigue
- persistent low mood outside the luteal phase
- dizziness or suspected iron depletion
The cycle may still matter. It just may not be the only thing that matters.
What to track
Track the same handful of symptoms each cycle, not a giant diary you will abandon:
- mood
- irritability
- bloating
- sleep
- pain/headache
- cravings
Ovelia is helpful here because PMS is the kind of repeating pattern people both undertrack and overdramatize. A clean monthly comparison beats a panicked memory every time.
The bottom line
If you want the evidence-first version of PMS supplement support, start with calcium, keep magnesium in the conversation when the pattern is tension/sleep-heavy, and stop expecting a one-cycle miracle.
The job is not to buy the most convincing bottle.
The job is to find the smallest intervention that makes the late-luteal week easier to carry, then confirm it over a real timeline.
That is how you build something useful instead of just repeating hope every month.
Sources:
Ready to track what actually works for you?
Ovelia turns what you read into a guided protocol you can actually follow.