Supplements for Libido in Women: What the Evidence Actually Says
Most supplements marketed for women's libido are much better at selling fantasy than producing reliable results. The practical move is to treat libido as a pattern, not a personality trait: match the supplement to the likely bottleneck, test one option at a time for 6 to 8 weeks, and track desire, arousal, comfort, and satisfaction instead of expecting one capsule to flip a switch.
 Low desire rarely looks dramatic from the outside. More often it feels private, layered, and hard to name clearly.
Low desire rarely looks dramatic from the outside. More often it feels private, layered, and hard to name clearly.
Low libido gets sold like a single-problem supplement category. It isn't.
Most women who feel less interested in sex are not dealing with one obvious deficiency that a capsule cleanly fixes. The pattern is usually layered: stress, fatigue, antidepressants, pain, hormonal shifts, sleep debt, relationship context, or simply a body that does not respond well to pressure. That is what makes the supplement conversation messy. There are a few compounds with real signal behind them. There is also a lot of overpromising built on tiny trials, narrow populations, and wishful thinking.
So the better question is not "what supplement increases female libido?" It is: in which situations do certain supplements seem to help, and what kind of help are we actually talking about?
What Most People Get Wrong
The biggest mistake is treating desire like a light switch.
Desire is more like a downstream readout of how safe, rested, hormonally supported, mentally present, and physically comfortable your body feels. That means a supplement can improve one part of the system without creating an instant Hollywood-style change in libido. Better lubrication is not the same as more spontaneous desire. Less sexual distress is not the same as wanting sex every night. More satisfying sexual encounters is not the same as fixing a relationship problem.
That distinction matters because the female sexual function literature is full of studies that show modest improvement on questionnaires, while the marketing version turns that into "works for libido."
There is another reason to be careful here: placebo response is unusually high in this category. A meta-analysis of female sexual dysfunction trials found that a large share of the measured treatment effect can be explained by placebo response alone. That does not mean nothing works. It means this is exactly the kind of topic where randomized, placebo-controlled trials matter more than anecdotes.
This is not a category with one universal winner. The better question is which supplement fits which pattern.
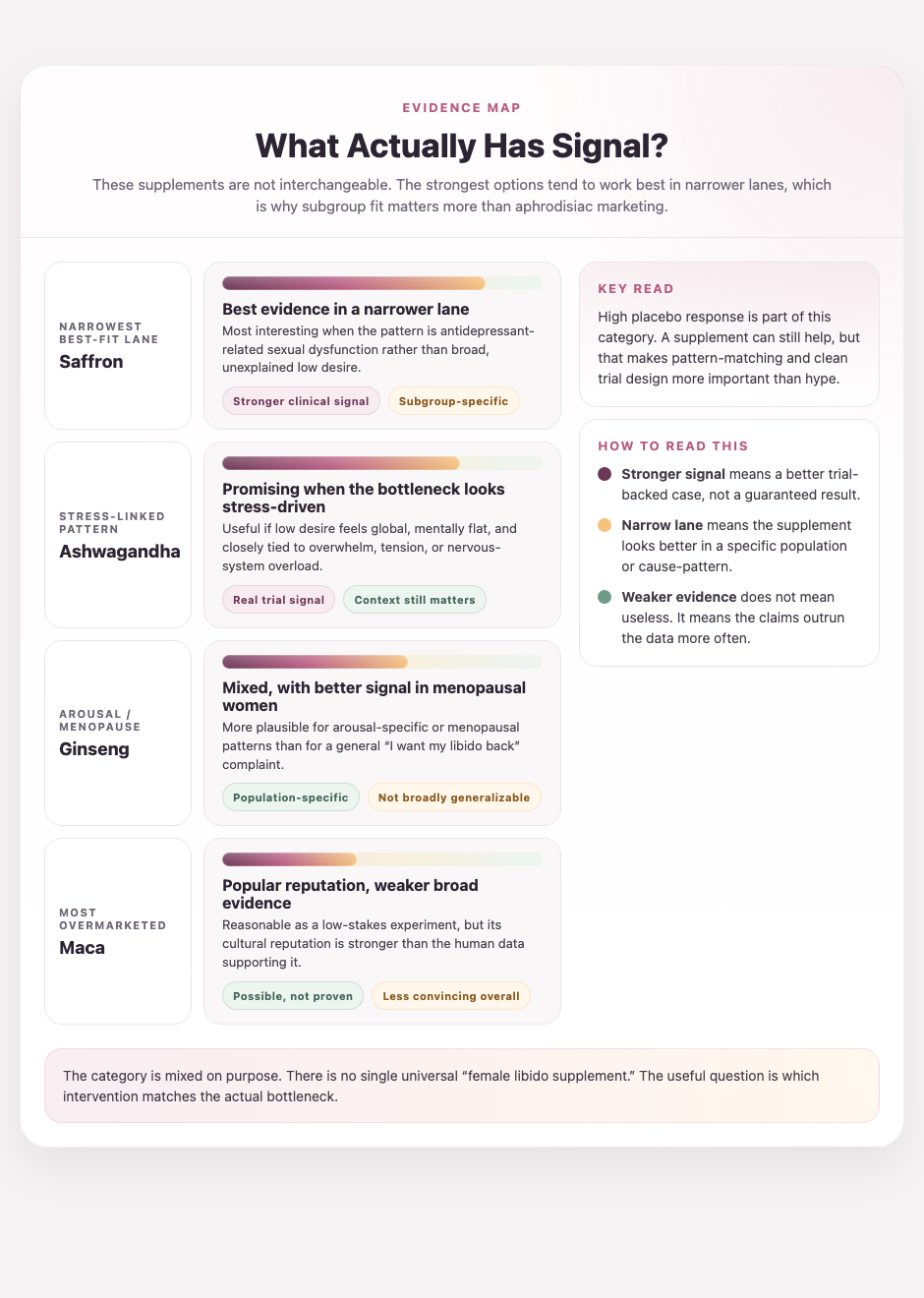
Where the Evidence Is Strongest
The cleanest way to look at this category is by pattern.
If stress is the obvious bottleneck, ashwagandha has some signal
Ashwagandha is one of the more plausible options when the pattern is chronic stress, mental load, and low desire that feels more shut-down than hormonal.
In a 2022 randomized, placebo-controlled trial, 80 women with low sexual function or high sexual distress took standardized ashwagandha root extract 300 mg twice daily or placebo for 8 weeks. The ashwagandha group improved more on the Female Sexual Function Index, the Female Sexual Distress Scale, and satisfying sexual encounters. The between-group separation was real, but this still does not mean ashwagandha is a universal libido fix. It means there is some evidence that it may help when the problem looks stress-linked and global rather than purely mechanical.
That mechanism makes intuitive sense. If your nervous system is running hot all day, desire usually loses.
If the context is antidepressant-related sexual dysfunction, saffron is more interesting than most people realize
Saffron has one of the more compelling evidence profiles in this category, especially in women dealing with antidepressant-related sexual side effects.
There is a 2022 three-center, double-blind, randomized, placebo-controlled clinical trial in women with sexual dysfunction showing saffron outperformed placebo in some domains, including desire, lubrication, and satisfaction. Earlier trials in women with fluoxetine-related sexual dysfunction also found improvement in several sexual-function domains over placebo.
That does not make saffron a broad recommendation for every woman with low libido. It does suggest that in the narrower lane of medication-related dysfunction, it deserves more respect than the usual "aphrodisiac" framing implies.
If the pattern is menopausal or arousal-specific, ginseng has mixed but non-zero evidence
Ginseng is one of those supplements that keeps showing up because the mechanism is at least plausible: blood flow, nitric oxide signaling, and possibly estrogen-related effects depending on the formulation and population.
The catch is that the results are uneven. A systematic review of placebo-controlled trials in menopausal women found positive evidence for sexual function overall, and Korean red ginseng appears to have the strongest signal in menopausal women specifically. But a placebo-controlled crossover trial in premenopausal women did not find a clear advantage over placebo on total sexual-function scores.
That is useful, because it tells you where not to overgeneralize. Ginseng may be more relevant for arousal and menopausal symptoms than for a vague "I want my libido back" complaint in otherwise healthy premenopausal women.
Maca is probably weaker than its reputation
Maca has a huge reputation in wellness culture and a much thinner human evidence base than most people assume.
The most relevant placebo-controlled trial in women looked at antidepressant-induced sexual dysfunction. Over 12 weeks, maca showed somewhat higher remission rates than placebo, with the signal appearing stronger in postmenopausal women. That is enough to call it promising in a narrow subgroup. It is not enough to treat maca like a proven general libido supplement for women.
This is the broader theme of the category: a supplement can be worth trying without being something the evidence strongly confirms.
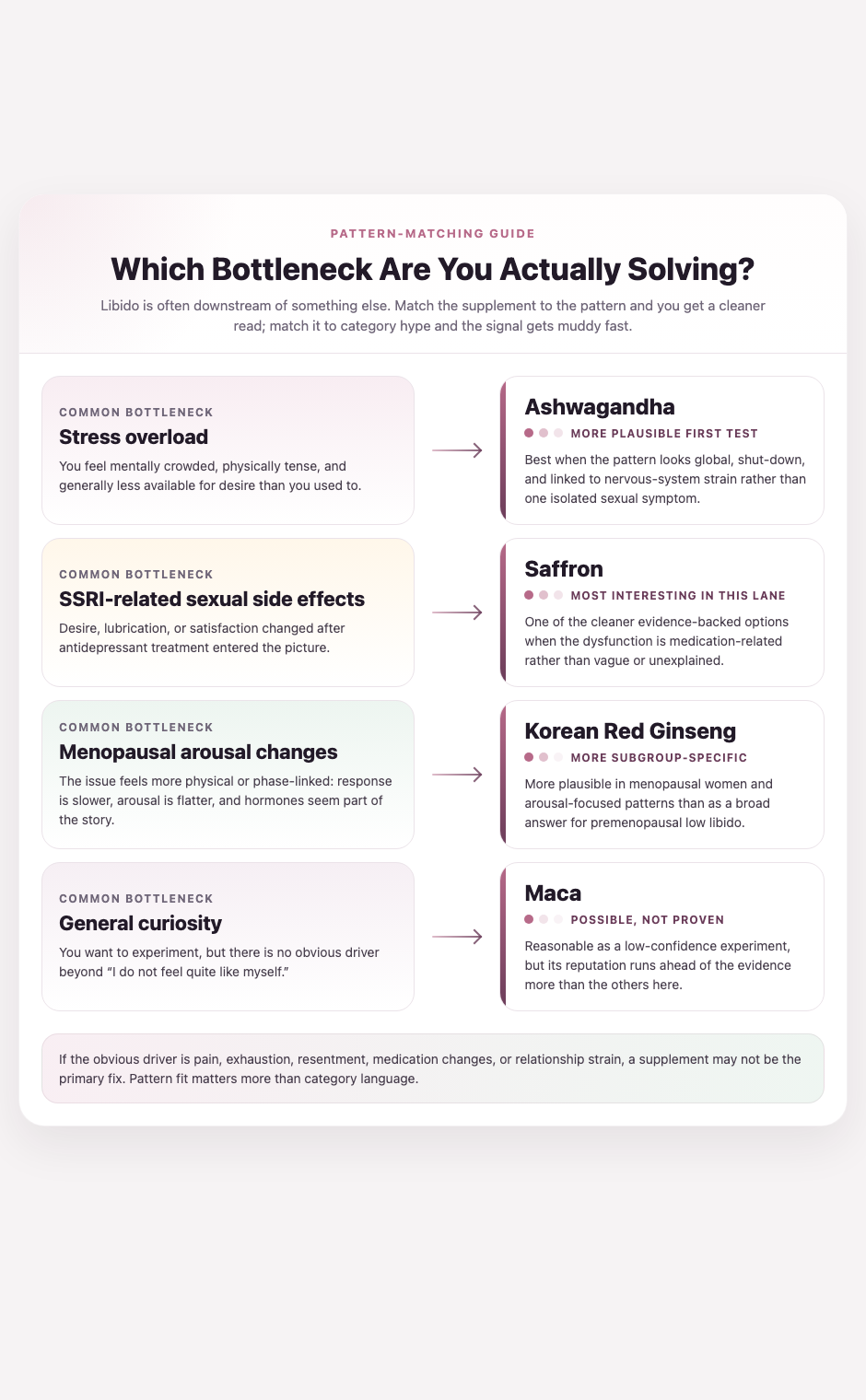
What This Means Practically
If you want to test supplements for libido without getting lost in marketing, match the supplement to the pattern:
- Stress-loaded, mentally flat, chronically "off": ashwagandha is one of the more reasonable first experiments.
- SSRI-related sexual side effects: saffron has some of the most interesting evidence in this lane.
- Menopausal arousal changes: Korean red ginseng is more plausible here than in younger, premenopausal women.
- General curiosity, weaker evidence, low downside: maca is more "possible" than "proven."
What I would not do:
- Start three "libido" supplements at once
- Assume more desire and more lubrication are the same outcome
- Treat a supplement as the answer when the obvious driver is pain, exhaustion, resentment, or medication side effects
- Expect a weekend-level change from a study that ran 8 to 12 weeks
This is also one of those categories where side effects and interactions matter more than the packaging suggests. Ginseng can interact with some medications. Saffron is not a free-for-all if you are pregnant or on medications where interactions matter. Ashwagandha is not for everyone, especially if thyroid issues, sedation, or GI side effects are already on the table. Libido supplements should be treated like interventions, not candy.
The useful move is pattern-matching, not buying the loudest “libido” bottle you can find.
What to Track
This is the kind of topic where memory will mislead you fast.
If you start a libido supplement, track four things for at least 6 to 8 weeks:
- Desire: how often you actually feel interested, not how often you think you should
- Arousal: whether your body responds more easily once you are in the moment
- Comfort: pain, dryness, or friction that changes whether sex feels inviting
- Satisfaction: whether the overall experience feels better, not just more frequent
Those are different outcomes. The best way to know if a supplement helped is to see which one moved.
If you are testing one of these, Ovelia is useful for exactly this kind of pattern reading. Not because libido needs more pressure or optimization language, but because the signal is subtle enough that a baseline matters.
The Bottom Line
Some supplements for female libido do have evidence behind them. Just not in the sweeping way the wellness internet suggests.
Ashwagandha has some signal in women with low sexual function and high distress. Saffron is genuinely interesting, especially for antidepressant-related dysfunction. Ginseng looks more population-specific, with the better signal in menopausal women. Maca is still more famous than proven.
The real takeaway is less sexy than the ads and more useful in real life: libido is usually a systems problem. The best supplement is the one that matches the actual bottleneck. If you do test one, test it slowly, one at a time, on a real timeline, with tracking.
That is how you figure out whether something helped your body, instead of just sounding promising on the bottle.
Sources:
- Beneficial effects of natural products on female sexual dysfunction: A systematic review and meta-analysis. Sultan S, et al. Phytotherapy Research. 2021.
- Crocus sativus (saffron) in the treatment of female sexual dysfunction: a three-center, double-blind, randomized, and placebo-controlled clinical trial. Journal of Psychosomatic Obstetrics & Gynecology. 2022.
- Efficacy and Safety of Ashwagandha (Withania somnifera) Root Extract for Improvement of Sexual Health in Healthy Women: A Prospective, Randomized, Placebo-Controlled Study. Ajgaonkar A, et al. Cureus. 2022.
- The Effect of Korean Red Ginseng on Sexual Function in Premenopausal Women: Placebo-Controlled, Double-Blind, Crossover Clinical Trial. Lee MS, et al. Journal of Ginseng Research. 2016.
- Ginseng for managing menopausal woman's health: A systematic review of double-blind, randomized, placebo-controlled trials. Kim TH, et al. Maturitas. 2016.
- A double-blind placebo-controlled trial of maca root as treatment for antidepressant-induced sexual dysfunction in women. Dording CM, et al. Evidence-Based Complementary and Alternative Medicine. 2015.
- Female Sexual Dysfunction: Natural and Complementary Treatments. Rapkin AJ, et al. Focus. 2018.
- Female Sexual Dysfunction and the Placebo Effect: A Meta-analysis. Bradford A, et al. Journal of Sexual Medicine. 2018.
Ready to track what actually works for you?
Ovelia turns what you read into a guided protocol you can actually follow.